Treatment
If bones directly affected by Paget's disease are painful, pain can often improve with treatment. Pain, however, can also arise from complications.
Bisphosphonates
Bones are made up of living tissue which is constantly being broken down and rebuilt by specialist bone cells. If this process is in balance, your bones should be healthy and strong. In Paget’s disease, this process causes the bone to become weaker and more likely to fracture. Bisphosphonates are drugs which work by inhibiting this bone remodelling process. These drugs reduce abnormal bone destruction by the osteoclasts, thereby restoring a more normal remodelling process.
Bisphosphonates help to strengthen your bones by improving their structure, which in turn reduces the risk of fractures. Bisphosphonates also help control bone pain. Note that it can take several months for bisphosphonates to have their full effect and for the individual to feel the maximum benefit. Bisphosphonates such as zoledronic acid (an infusion into the bloodstream) and risedronate (tablets) are the most commonly used to treat Paget’s disease.
- The current first-line bisphosphonate used to treat Paget’s disease, is zoledronic acid
Zoledronic acid
Zoledronic acid (also known as zoledronate), a bisphosphonate is considered the first-line treatment for Paget’s disease, due to its potency and prolonged duration of action. Products containing Zoledronic acid are known by brand names such as Aclasta and Reclast. Zoledronic Acid is the bisphosphonate most likely to relieve pain from active Paget’s disease.
It is usually given in hospital, as an outpatient, although some GP surgeries may occasionally give it. A single dose of 5mg is given through a drip (infusion) directly into a vein in your arm (intravenous) and usually takes around 15 to 30 minutes. Over the following months, this treatment often normalises the abnormal bone remodelling and, for Paget’s disease, one single dose can be effective for many years.
Alternatives to zoledronic acid
Bisphosphonates can also be given as tablets; these are slightly less effective than an infusion of zoledronic acid, at reducing bone remodelling, and the effect doesn’t last quite as long.
Risedronate
The most commonly used oral bisphosphonate is 30mg of risedronate sodium, taken daily, for two months. If necessary, the course can be repeated.
Why the instructions matter
To ensure risedronate is absorbed properly, it should be taken with a full glass of water, on an empty stomach, first thing in the morning. It is important that you do not take it with food, other medicines or drinks (other than plain water). If taken at the same time, medicines containing any of the following lessen the effect of risedronate: calcium, magnesium, aluminium (e.g. some indigestion mixtures) or iron.
Tablets like risedronate can sometimes irritate the oesophagus (the tube that carries food to your stomach). To help prevent this, it’s important to take them in a way that lets the tablet move quickly into your stomach and stay there while it dissolves.
How to take the tablet safely
• Sit upright or stand to take the tablet and for at least 30 minutes after taking it. This helps the tablet travel straight down into your stomach and reduces the chance of it getting stuck or causing irritation on the way down.
• Wait at least 30 minutes before eating or drinking anything other than water and before taking any other medicines or supplements. This gives your body time to absorb the tablet properly.
• Avoid bending over or lying down until after you’ve had your breakfast. This helps prevent the medication from washing back up into your oesophagus, which can cause irritation.
Pamidronate
Pamidronate is an effective treatment but has largely been superseded by zoledronic acid which lasts longer and is easier to administer. Pamidronate is given in several doses, intravenously (an infusion into the bloodstream), and repeated when necessary, dependant on symptoms. Doses can vary, but commonly 60mg is given by an infusion over a period of four hours and this is repeated on three consecutive days.
Calcitonin
In some cases where bisphosphonates are not recommended, calcitonin injections may be considered to treat bone pain in Paget’s disease.
What about side effects of bisphosphonates?
A comprehensive review on the effects of bisphosphonates in the treatment of Paget’s disease, published in 2017, concluded that serious side effects were rare and that the most common side effects experienced were a flu-like illness in people given bisphosphonates by infusion, and stomach upset in those given tablets. Severe side effects causing treatment discontinuation were rare.
The most common side effect with zoledronic acid is a flu-like reaction that lasts a day or two in most people who experience it. It is usually of mild or moderate severity, but more severe reactions can sometimes occur. Pamidronate can also cause a flu-like reaction but there is less information on the frequency with which this occurs or its severity. If a flu-like reaction does occur with either drug, it can usually be controlled with paracetamol or ibuprofen. Both Zoledronic acid and pamidronate may cause a decrease in calcium levels. The risk of this is reduced in people who have a good dietary calcium intake and those with normal levels of vitamin D. Calcium and vitamin D levels (25-hydroxy vitamin D) might be measured before treatment to determine if supplements are required. Depending on the results, calcium and vitamin D supplements may be given prior to treatment as a preventative measure.
The most common side effect of taking risedronate is stomach upset.
On rare occasions, bisphosphonates are associated with osteonecrosis of the jaw (ONJ). This is a condition which may present after dental surgery when exposed bone fails to heal. ONJ is rarely seen in those with Paget’s disease and the risk of ONJ is greater if bisphosphonates are given for cancer. As a precaution, however, if possible, complete any extensive dental treatment prior to bisphosphonate treatment. If you have to undergo extensive dental procedures, it is important to inform your dentist that you are having, or have had treatment with a bisphosphonate. You will find some information here (external website).
The patient information leaflet that comes with your medication has the full list of potential side effects and your healthcare team can talk through anything you’re unsure about or worried about.
Most people who need bisphosphonates find them beneficial. While side effects can happen, your doctor will look at your individual circumstances and help you weigh things up. When treatment is recommended, the benefits of protecting your bones often outweigh the risks of any potential side effects.
When should bisphosphonates be avoided?
The decision to give treatment may be modified if you have another medical problem which could be aggravated by bisphosphonates. As bisphosphonates are excreted by the kidneys they cannot be used if there is significant kidney disease. If you are being considered for bisphosphonate treatment, the doctor will usually organise a blood test to check kidney function, to see if it is safe to go ahead. Although bisphosphonates are rarely given to younger people, they should be avoided during pregnancy as their effects on the foetus are unknown.
Follow up
An assessment of the response to treatment should take place between 3 and 6 months after the treatment has been completed.
Clinical guideline
A clinical Guideline, for the diagnosis and management of Paget’s Disease of Bone in adults, was commissioned by the Paget's Association. The full Guideline was published in the Journal of Bone and Mineral Research. It has been endorsed by the European Calcified Tissues Society, the International Osteoporosis Foundation, the American Society of Bone and Mineral Research, the Bone Research Society (UK), and the British Geriatric Society. Read more here
Other medication
Analgesics
Although bisphosphonates can help reduce bone pain, some patients require a painkilling drug (analgesic) for maximum pain relief, particularly if there is significant osteoarthritis in major joints. Analgesics which are commonly used include paracetamol, co-codamol and dihydrocodeine or non-steroidal anti-inflammatory drugs such as ibuprofen.
- See our booklet ‘Paget’s Disease and Pain’
Calcium and vitamin D
Calcium is vital for the development of healthy bones, whilst vitamin D is required to help regulate the way your body uses calcium, and to ensure your bones, muscles and teeth remain strong. Calcium is in foods such as milk and cheese, broccoli and cabbage, and soya beans. Additional calcium may be required if an individual has a low intake of dairy produce.
Vitamin D is mostly obtained by the action of sunlight on your skin, but it is also in foods such as oily fish. In the UK from October to March, we cannot make vitamin D in our skin therefore, some people might not have enough to last through the winter and may need a supplement to boost their diet. Advice given by Public Health England in 2016, was for everyone to have a daily supplement of 10 micrograms (which is equal to 400 International Units) of vitamin D. This was a general recommendation for everyone, as it is difficult to know who receives enough sunlight exposure to produce vitamin D, and also to cover those at risk of deficiency. Most supplements contain vitamin D3 (cholecalciferol) which may be slightly more effective than vitamin D2 (ergocalciferol).
As discussed earlier, treatment with zoledronic acid or pamidronate may cause some patients to have low levels of calcium in their blood. Calcium and/or vitamin D supplements may be prescribed prior to treatment.
Is surgery required?
Surgery may be required to treat complications of Paget’s disease such as fractures, osteoarthritis and when bone enlargement is thought to be compressing the nerves in the spine. Prior to surgery, it is usual for bisphosphonate treatment to be administered in the hope that this might reduce blood loss, which can occur in Paget’s disease, due to the increased vascularity of affected bone.
Surgery may be required under the following circumstances:
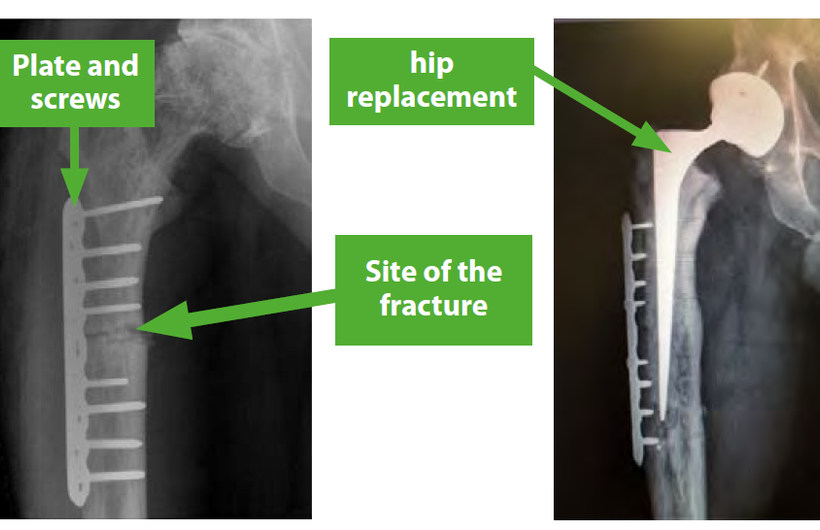
- If an affected bone fractures (breaks), an operation is usually necessary to stabilise the fracture (lefthand image below).
- When Paget’s disease leads to marked damage of the joints (osteoarthritis) and if symptoms and disability from this become severe, joint replacement surgery may be required (righthand image below).
- When there is marked bone deformity, usually seen in the lower leg, an osteotomy can be carried out. This involves breaking the bone and realigning it to correct the shape.
- If nerve compression occurs, surgery may be necessary, e.g. Paget’s disease in the spine can press on the spinal cord, causing a narrowing that occasionally needs to be corrected surgically, if medical treatment is unsuccessful.
March 2026
Facts about Paget's disease
Paget's Nurse Helpline
Contact the Paget's Nurse Helpline for information and support on all aspects of Paget’s disease
Membership
Become a member of the Paget's Association
Join today to unlock a world of insights into Paget's disease and support our cause.
As a valued member, you'll receive a comprehensive Paget’s Information Pack, along with our regular Paget's News magazine.
Stay at the forefront of advancements with our latest news: research, treatment and more.
Don't miss out – explore the benefits of membership now!